[Levitan, L., LaBerge, S., DeGracia, D.J. & Zimbardo, P.G. (1999). “Out-of-body
experiences,” dreams, and REM sleep. Sleep and Hypnosis, 1(3), 186-196.]
Corresponding author: Stephen LaBerge, Ph.D. Department of Psychology, Stanford
University, Stanford, CA 94305-2130. Email: slab@psych.stanford.edu
Lynne Levitan [University of California, Davis, School of Medicine],
Stephen LaBerge [Department of Psychology, Stanford University],
Donald J. DeGracia [Department of Emergency Medicine, Wayne State University]
and Philip G. Zimbardo [Department of Psychology, Stanford University]
Abstract
An out-of-body experience (OBE) is characterized by the sensation of leaving the physical
body and functioning independently of it. Such sensations also occur during some lucid
dreams. Some authors aver that OBEs and lucid dreams are completely different
phenomena. The present investigation tested an explanatory model of OBEs as a form of
dreaming similar in nature to lucid dreaming.
Study 1 consisted of scored content analysis on 107 lucid dream (LD) reports verified by
eye movement signals during REM sleep. Ten LD reports (9.3%) from 5 of the 14 subjects
qualified as OBEs. LDs initiated from brief REM awakenings were significantly more
likely (4.4 times, p<.02) to be judged as OBEs than LDs initiated during uninterrupted
REM sleep.
Study 2 was a survey of 604 subjects assessing the frequency of reported OBEs and
dream phenomena. Frequent OBE reporting was related to frequent reporting of dreams
and dream-related events; frequency of OBE reporting was significantly lower than lucid
dream reporting, and similar to that found in the laboratory in Study 1.
These studies support the close association of OBEs and lucid dreaming. REM sleep
and states favorable to OBEs share the feature of high CNS arousal under sleep or sleeplike
conditions. Such states are conducive to the generation of somatosensory
hallucinations interpretable as the experience of rising “out-of-body.” The discussion
highlights the importance of semantic interpretations of such experiences, and presents a
three-part model for analyzing “metachoric” experiences such as lucid dreams and OBEs.
Further discussion considers the role of cortical activation in the generation of OBEs
and lucid dreams. The conclusion argues that all states of consciousness, sleeping or
waking, derive from the same basic brain functions, which act to model the world based on
perceptual maps. OBEs, dreams, and the reality experienced in the waking state are all
mental constructions, and further efforts in consciousness research may benefit from
avoiding an arbitrary distinction between sleeping, dreaming and waking states.
An “out of body experience” (OBE), is characterized by the perception that one's locus of
awareness has separated from the physical body(1). According to surveys, 5-35% of people
report having had an OBE at least once in their lives (2).
OBE-type events have surely been part of the human experience for time immemorial.
Nineteenth century occultists are responsible for the first known attempts to place these
experiences within a theoretical framework. The original occultist formulation of the OBE
held that human consciousness can separate from the body and travel in nonphysical
realities, so-called “astral projections” (3, 4; for historical reviews see 5, 6). Later authors
modified the theory, asserting that the discorporate consciousness was capable of
traveling in the physical world (7, 8).
Contemporary scientific thinkers consider OBEs to be complex hallucinatory
experiences (2, 9). The consistency of phenomenology (10) across experiences and
individuals suggests that a common set of events underlies the OBE. To the occultists and
the naive thinker, the literal interpretation of consciousness leaving the body is the
commonality. For the model of the OBE as an hallucination to have explanatory power
requires postulating a specific set of internal events common to individuals experiencing
OBEs. Potential sources of the predilection to have OBEs are: personality,
psychopathology, mental or physical trauma, or a natural extension of ordinary
psychological processes. The data presented here support the latter idea.
A number of writers have proposed that OBEs are evidence of psychological
dysfunction. For example, Freud wrote that OBEs are hallucinations resulting from
infantile complexes, and other authors have suggested that OBEs occur as defense
reactions to guilt, stress, grief, or as a symptom of psychopathology (11, 12). The DSM-IV
(13) includes out-of-body feelings (“...a sensation of being an outside observer of one's
mental processes, one's body, or parts of one's body”) within the diagnostic criteria for
depersonalization disorder (p. 488).
However, there is little indication of any substantial correlation between
psychopathology and OBEs. Gabbard and Twemlow (14) compared measures of
psychological adjustment in people who reported OBEs with those from various other
groups, including psychiatric patients. They concluded that the OBE group represented “a
very close approximation of the 'average healthy American.'” (p. 31)
More recent neurocognitive theories offer an alternative to literal and pathological
explanations of OBEs. Blackmore (1, 2) and LaBerge (15-17) have suggested that OBEs can
result when real-time sensory input from the external environment and body is lost and
is replaced by internally generated perceptual constructs. In support of this model is a
growing body of data describing perceptual and cognitive “maps” operating at multiple
levels of the central nervous system (18-20). Activation of these maps could support
conscious, perceptual and cognitive activity in the absence of sensory input (21). This
would explain how the mind can create fully realistic perceptions of a “out-of-body” body
and an external world in circumstances in which conscious cognition persists despite the
loss of externally provided sensory data. As discussed below, this theory additionally
explains the typical phenomena at the initiation of an OBE and the sensation of lifting out
of the physical body.
The juxtaposition of consciousness and diminished sensory input is not a rare event. It
occurs several times a night in normal REM sleep. In this state, the sleeping mind creates
vivid sensory experiences without data from external environment or the sleeper’s body,
and the dreamer thinks about and acts upon these perceptions (22). In fact, the perceptual
aspects of OBEs and dreams are similar in the sense of being what Green and McCreery
term “metachoric experiences” (9), “in which the normal perceptual environment is
entirely replaced by a hallucinatory one, which may on occasion be a convincing replica
of the world of normal perception” (p. 56). As further elaborated below, the mechanisms
underpinning OBEs and dreams are likely to be the same as those responsible for normal
conscious experience, thus accounting for the extraordinary verisimilitude to waking
reality described in reports of OBEs and dreams (23).
A primary difference between typical dreams and OBEs is that the world perceived in a
dream is not usually a representation of the sleeper's current physical environment. This
may be one reason why many people say that OBEs feel more real than dreams (14). The
reason for the continuity of experience in OBEs is likely to be the direct transition from
normal perception of the external environment to a state of dissociation from sensory
input, without an intervening period of unconsciousness such as usually occurs in sleep.
Other common aspects of the experience include “electrical” sensations, vibrations,
loud rushing sounds, and a feeling of heaviness or bodily paralysis that precedes the
feeling of “leaving” the body (4, 14, 24, 25). These strange sensations are remarkably
reminiscent of descriptions of a phenomenon observed by sleep researchers, referred to as
“sleep paralysis.” Sleep paralysis generally occurs during sleep onset, particularly under
conditions of sleep deprivation, when one is more likely to enter REM sleep directly from
waking. The individual is usually in bed, (except in the notable case of narcolepsy in
which the sudden onset of catalepsy during waking activity is a classic symptom of the
disease) (28). As the individual falls asleep, the skeletal muscle atonia of REM sleep
manifests and is perceived consciously, while the sleeper maintains continuous
conscious cognition (26). Again, no state of diminished awareness such as non-REM sleep
has intervened between waking and sleep. To an observer, the person appears to be asleep,
yet the sleeper’s experience is of being awake but paralyzed and, in some cases,
experiencing unusual auditory, tactile, or visual perceptions.
Everett (27) collected descriptions of sleep paralysis from a group of 52 medical
students (an excellent population for the study of sleep deprivation!), eight (15%) of whom
reported having had the experience. The subjects reports included phrases such as, “I feel
completely removed from myself,” “feeling of being separated from my body,” “eerie,
rushing experiences,” hearing “hissing in the ears,” and “roaring in the head.” Fear was
also a common component of the subjects' paralysis experiences.
The parallels between the phenomena suggest that at least some OBEs arise from
conditions similar to sleep paralysis, and that the two terms may actually be naming
different aspects of the same phenomenon. Corroboration of this hypothesis comes from
investigation of the circumstances in which OBEs occur.
Because there is no clear subjective transition between waking and sleeping during
sleep paralysis, subjective reports are not always helpful in determining if an OBE has
occurred during sleep onset. Lack of awareness of entering REM sleep would lead the
sleeper to believe that subsequent events occur in the waking state. However, the
literature also supplies indirect clues in the form of information on what percentage of
OBEs arise in states potentially conducive to sleep and sleep paralysis, for instance, while
resting or lying down.
In one survey, 85% of people claiming to have had OBEs said they had occurred during
resting, sleeping or dreaming (29). Other surveys also showed that the majority of OBEs
happen when people are in bed, ill, or resting, with a smaller percentage associated with
being drugged or medicated (1, 30, 31).
Not all OBEs occur during sleep or sleep onset. Some people who can deliberately
induce OBEs appear to do so in hypnagogic or auto-suggested trance states (32), and OBEs
no doubt arise in other states of consciousness as well. Nonetheless, certain essential
features may be characteristic of all states in which OBEs occur. Among these are likely to
be: loss of proprioceptive input from the body and visual and tactile input from the
external environment, as these sensory modalities locate our awareness in space;
continuity of conscious cognition during the period of loss of sensory input; and profound
muscular relaxation or paralysis leading to a sensation of heaviness in the physical body.
Muscular relaxation similar or identical to the atonia of sleep paralysis can occur during
hypnosis and following anesthesia (33, 34), and profound relaxation also may be
sufficient to reduce proprioceptive input. Intense focus of attention (as in hypnosis) or
psychoactive substances (such as dissociative anesthetics) can attenuate exteroceptive
sensory input.
Several studies have examined whether those who report OBEs are also more likely to
report dream-related phenomena, such as lucid dreams (dreaming while knowing one is
dreaming), falling and flying dreams, and hypnagogic imagery (24). Eight of ten of these
studies showed a significant positive relationship between the reported frequency of lucid
dreams and OBEs. Blackmore found a statistically significant association between an
individual's claim of having had OBEs and high reported frequencies of hypnagogic
imagery, falling dreams, flying dreams, false awakenings and dream control (willful
alteration of the events of a dream) (1, 29). Glicksohn (35) found that individual OBE
incidence correlated positively with the incidence of hypnopompic (but not hypnagogic)
imagery, flying dreams, falling dreams, the ability to discontinue dreams, and lucid
dreams.
Thus, there is a background of evidence supporting a relationship between the
tendency to experience OBEs and a variety of dream-related phenomena. The studies
discussed here support a specific relationship between REM sleep and OBEs. These studies
derived from an observation that arose in the context of research on lucid dreaming. In a
laboratory study of the onset of 76 lucid dreams from 13 subjects, approximately 10% of the
lucid dream reports collected included descriptions of events such as lying in bed, feeling
strange bodily sensations (often vibrations), hearing loud humming noises, and rising
“out of body” to float above the bed.
The study, which utilized LaBerge's eye-movement signaling methodology to mark the
time of lucidity onset (16, 36, 37) revealed that lucid dreams have two modes of initiation.
In the more common variety, the “dream-initiated lucid dream” (DILD) the dreamers
acquired awareness of being in a dream while being fully involved in it. DILDs were
initiated in a state showing all of the physiological signs of REM sleep: suppressed muscle
tone, low-amplitude, mixed-frequency EEG, and intermittent burst of rapid eye
movements (38).
DILD-type lucid dreams accounted for 72% of the signal-verified lucid dreams. In the
other 28%, dreamers reported awakening from a dream and returning to the dream state
with unbroken awareness -- one moment they were aware that they were awake in bed in
the sleep laboratory, and the next moment they were aware that they had entered a dream
and were no longer perceiving the room around them. Entry into these “wake-initiated
lucid dreams” (WILDs) shared many features of sleep paralysis (17). A preliminary
examination of the dream content and physiological records suggested that OBE-type
dream content was more common in WILDs. Study 1 was a test of this hypothesis by
retrospective analysis of the data set just discussed.
Study 1
Method
Subjects The 14 volunteer subjects (7 men, 7 women) ranged in age from 18 to 38. The
selection criteria were: freedom from sleep disorders, excellent dream recall (more than
one dream recalled per night), frequent lucid dreams (on the order of one per week or
more), and interest in lucid dreaming. The subjects were all trained in various luciddream
induction methods (15, 16).
Procedure Subjects spent from 2 to 25 non-consecutive full nights sleeping in the
laboratory. Physiological data collection included standard polysomnograms [i.e.,
electroencephalogram (EEG), electro-oculogram (EOG), and submental electromyogram
(EMG)] (38), and, in some cases, additional physiological measures not reported here.
Before bedtime on recording nights, subjects received instruction to signal, by means
of eye-movements, immediately upon realizing that they were dreaming. The type of
signal specified varied somewhat; the most common was two pairs of extreme horizontal
eye movements (i.e., left, right, left, right). In some cases, subjects had additional
instructions for carrying out specific activities in the dream state after attaining
lucidity.
The protocol further instructed the subjects to write reports on the content of their
lucid dreams immediately upon awakening from the REM period in which they occurred.
The reports were to contain descriptions of when the subjects had made eye-movement
signals, as well as how they recognized they were dreaming and the other events of the
dreams. Correlation of the eye-movement signals identified on the polygraph recordings
with those described in the reports enabled accurate identification of the time of onset of
lucidity on the physiological record.
Measures A judge blind to the report classifications (WILD or DILD) scored the
subjective dream reports on four dichotomous content scales:
1. OBE. Scored as present if the report mentions leaving the body, e.g., “I was floating
out of body” “I...felt that I had left my body” “I...sense that I’m floating
out of my body”.
2. Body distortion. Scored as present if the report mentions distortion of body
(including paralysis or vibrations).
3. Reference to bed. Scored as present if the report mentions being in bed, being asleep,
or lying awake in the laboratory.
4. Flying. Scored as present if the report mentions floating or flying.
A second judge scored a random sample of 20% of the reports. The two judges agreed
perfectly on all four content scales for this sample, indicating a high degree of reliability
of the measures.
An experienced sleep technician had scored the polygraph records for sleep stages
according to standard procedures (38). In addition, a simultaneous analysis of the
physiological records and corresponding subjective reports for each lucid dream
dichotomously classified them as either WILDs or DILDs. For a dream to meet the criteria
for a WILD, less than two minutes of REM could intervene between the last period of
wakefulness (as assessed on the physiological record) and the eye-movement signal
denoting lucidity onset, and the subject must have reported entering the lucid dream
directly from the waking state without loss of awareness. The criteria for a DILD specified
that more than two minutes of REM or other stage of sleep had preceded the eye movement
signal and the subject had reported becoming lucid while already involved in a dream.
Results
The 14 subjects reported signaling lucidity onset in dreams in 113 separate REM
periods. In 107 cases (95%), correspondence of eye-movement signals on the polygraph
record with subjective lucid dream reports verified the reported time onset of lucidity
(SVLDs). Eighty-seven (81.3%) of the 107 SVLDs met the criteria for classification as
DILDs, and twenty (18.7%) as WILDs. Ten reports (9.3%) from five of the subjects contained
specific references to out-of-body experiences, e.g. “I felt myself leaving my body.” Five of
the twenty WILDs (25%) were OBEs versus five of the eighty-seven DILDs (5.7%) (Fisher's
Exact Test, p <. 019). OBE content was 4.4 times more likely to occur in WILD reports than
DILD reports. The odds of a WILD being classified an OBE was 0.333; the odds of a DILD
being classified an OBE was only 0.061. The odds ratio for the occurrence of an OBE in the
context of a WILD compared to in the context of a DILD was 5.5 : 1. The definitive OBE
phrase (“I felt myself leaving my body”) occurred exclusively in initial scenes of the lucid
dream reports.
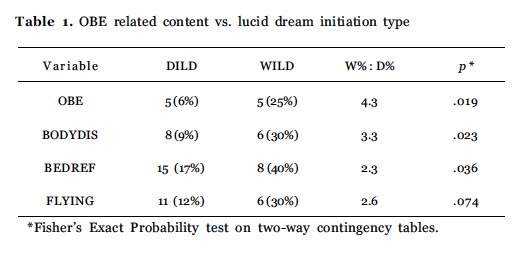
The three OBE-related experiences, body distortion, floating or flying, and reference to
bed, all appeared more often in WILD than in DILD reports (see Table 1). Of WILD reports,
six (30%) contained body distortions, six (30%) included flying, and eight (40%) included
references to being in bed. In contrast, just eight (9%) of DILD reports contained body
distortions, ten (12%) included flying, and 15 (17%) included bed references.
The experiences described in the five DILD reports classified as OBEs closely resembled
events from WILD reports in that the subjects reported feeling themselves lying in bed and
experiencing strange sensations such as paralysis and floating out of body. Although the
subjective reports of each of these DILDs had met one WILD criterion by describing the
subjective experience of direct and conscious entry into a dream after a period of perceived
wakefulness, they did not meet the physiological criterion of exhibiting signs of
wakefulness in the two minutes immediately preceding the lucidity signals. However, it
is possible that the subjects could have become aware of their environments and bodies
very briefly (and hence been perceptually “awake”) while continuing to show the
brainwaves and low muscle tone normally associated with REM sleep.
Study 2
The second study was a survey designed to assess the applicability of the first study’s findings in the sleep laboratory (in vitro) to events occurring in the more natural environment outside the laboratory (in vivo). The hypothesis for this investigation was that OBE frequency would be associated with increased frequency of certain unusual sleep and dream phenomena. The survey also included questions to test a secondary hypothesis, based on indications from the first study that physiological circumstances favorable for OBEs in REM sleep (awakenings followed by return to REM sleep with continuous awareness) occur rarely, that OBE reports would be less frequent than lucid dream reports.
Method
Subjects A total of 604 subjects, from three samples, completed the questionnaires. Stanford University undergraduates in an introductory psychology course made up two of the samples. The third sample consisted of 136 readers of the NightLight, a newsletter about lucid dreaming research.
Procedure The students completed the questionnaire in partial fulfillment of a course requirement to participate as a subject in psychology department experiments. The newsletter solicited responses to the questionnaire with an appeal for assistance in enhancing scientific understanding of lucid dreaming. None of the subjects received any remuneration.
The mean age in the two student groups was 19 years; the mean age of the NightLight group was 41. Forty-five percent of the participants were women.
Measures The questionnaire inquired about the frequency with which the respondents had experienced various events. Subjects selected one of twelve different frequency levels for dream recall, lucid dream frequency, frequency of returning to a dream after an awakening and OBE frequency. The incidence of sleep paralysis was assessed with a yes or no question. The data from 32 subjects (5.3%) were dropped from the analysis because of unanswered questions or internal consistency errors (such as reporting a higher rate of recall of lucid dreams than of all dreams). A total of 572 valid questionnaires remained.
Results
Of the subjects in the three groups combined, 34.2% (196) reported having had an OBE at least once, while significantly more, 81.8% (452), claimed to have experienced lucid dreams. The student groups both reported dream recall with a median frequency of 3 to 4 per week, while the NightLight group (highly interested in dreams) reported a median of 1 per night.
For the entire sample, median frequencies were: dream recall 3 to 4 dreams times per week, lucid dreams 4 times per year, and dream return 4 times per year. More than half of the subjects reported no OBEs in their lifetimes. Over a third (37.1%, 212) reported experiencing sleep paralysis and 84.5% (483) had been able to return to a dream after awakening.
The reported frequencies of the dream-related experiences and OBEs were significantly related. Subjects were more likely to report having had one or more OBEs if they also reported having had lucid dreams (38.5% or 174 of 452), than if they reported never having had a lucid dream (15%, Chi-square = 20.7, p < .0001). Subjects reporting dream return showed a higher incidence of OBEs (35.8%), than subjects not reporting dream return (20%, Chi-square = 8.9, p < .003). Subjects who had experienced sleep paralysis showed a higher likelihood of also having had OBEs (44.2%) than subjects who had never experienced sleep paralysis (28%, Chi-square = 15.4, p < .0001).
The dream experience variables interacted with each other in affecting the rates of OBE incidence. Subjects who reported having had lucid dreams, dream return and sleep paralysis (N = 324) were the most likely to have also experienced OBEs (51%, 165). The highest frequencies of OBEs per dream also came from this group (N = 165, F = 4.5, p < .05). The OBEs per dream measure served to control for the effect of dream recall on reported OBE frequency. This was necessary because an ANOVA of OBE frequency by dream recall category (low < 30 dreams per year, medium < 172 dreams per year, and high > 446 dreams per year) showed that increasing rates of dream recall were significantly related to increasing rates of OBE occurrence (N = 580, F = 10.2, p < .0001). Thus, the OBEs per dream measure demonstrates that the subjects who reported all three dream related events were in fact more likely to have experienced OBEs, and that their reporting of OBEs was not an artifact of high levels of dream recall.
In a multiple regression on the OBEs per dream variable (transformed to achieve normality), sleep paralysis (two levels), lucid dream frequency (transformed to normality), and dream return frequency (transformed to normality) together predicted OBE frequency (p < .01). In single regressions, lucid dreams per dream (a derived variable that corrects for dream recall) correlated with OBE frequency (r = .18, t = 4.35, p < .0001), as did dream return frequency (r = .12, t = 2.80, p < .005). The small (but statistically significant) size of these correlations probably resulted from the large amount of “noise” inherent in the survey studies.
Dream return frequency per dream, a variable which by logic should be related to the tendency to experience wake-initiated lucid dreams, correlated positively and significantly with lucid dreams per dream on a Spearman test (ρ = .215, p <.0001). Lucid dream frequency, as expected, correlated with dream recall (N = 579, ρ = .40, p <.0001).
In the first study, WILDs occurred at about 10% of the frequency of DILDs, and according to the second study hypothesis, OBE frequencies should be correspondingly lower than lucid dream frequencies. That is, the predicted OBE frequency should be about 10 times less than the observed lucid dream frequency. The median lucid dream frequency for the entire group was 4 per year, so the predicted median frequency of OBEs is 0.4 per year, a figure consistent with the observed frequency of 0.5 OBEs per year in the NightLight group. This analysis was not possible for the whole group as the group median OBE frequency was zero. In a paired t-test on the entire group comparing observed OBEs per year with the predicted value for OBEs per year (lucid dreams per year divided by 10), the difference between theory and observation was not significantly different from zero (N=565, t = 1.13, p < .25).
Study 2 Discussion
The results from Study 2 indicate clearly that people who report certain sleep and dream related experiences are more likely also to report OBEs than people who do not. Subjects in the current study who reported lucid dreams were 158% more likely to report OBEs than subjects who did not report lucid dreams. Those reporting dream return reported OBEs 85% more often than others, and those reporting sleep paralysis reported OBEs 59% more often. The results of this survey study corroborate those of previous authors (1, 24, 29, 35), demonstrating that the tendency of subjects to report OBEs is strongly related to the frequency of with which they report dream-related events.
Olson (39) also reported finding that people who reported OBEs claimed a higher frequency of dream recall than non-reporters. However, other researchers have not found this association (29, 35). Previous investigations may not have established this correlation because the levels used to assess dream recall reach a ceiling at a fairly low level of recall.
General Discussion
The strong association between OBEs and REM phenomena suggests that the physiology of REM sleep occasionally provides conditions conducive to experiences like OBEs. In particular, the occurrence of wakefulness immediately prior to entry into REM sleep appears to enhance the likelihood of OBE-like dream content. Study 1 supported this observation by demonstrating that “OBE” lucid dreams and lucid dreams containing OBE-like content were most common in wake-initiated lucid dreams (WILDs). Study 2 added further weight by revealing correlations between OBE frequency and the frequency of events associated by definition with awakenings during the REM state: sleep paralysis and dream return.
A fully reasonable conclusion is that out-of-body experiences are mental phenomena that arise out of a specific set of physiological and sensory events that sometimes occur during the transition from waking to REM sleep. The common term for mental phenomena associated with REM sleep is “dream.” By this logic, OBEs occurring during REM sleep are dreams.
However, it is clear that OBEs are not typical dreams. Perhaps the most salient distinguishing characteristic of these episodes beyond the basic phenomenon of feeling “out-of-body” is the tenacious belief of OBE enthusiasts that the experiences are “not dreams.” People who have had an OBE commonly report that the experience seemed “more real” than dreams, and that they were certain that they were not dreaming during the event.
The recognition that one is dreaming results in lucid dreaming, which accounts for a very small minority of dreams. All of us dream every night, and in general we are fully convinced of our wakefulness during our dreams, regardless of what fantastic or outrageous events transpire. Therefore, the assertion that one is certain one is not dreaming carries little weight without proof. In addition, the superior “reality” claimed for OBEs is reminiscent of the experiences of first-time lucid dreamers who frequently reflect on how astonishingly real or solid the dream world seems.
With more careful scrutiny, the feature of the OBE that distinguishes it from ordinary dreams is the presence of cognition reflecting on the nature of the experience. This feature is shared with lucid dreams, in which the dreamer reflects on the fact that the experience is a dream. Thus, the only difference between the lucid dreams in Study 1 in which the subjects experienced floating out of their bodies and the OBEs reported by people who believe they are literally “out-of-body” (7, 40) is the belief of the individual having the experience. In both cases, the individual reflected on the experience: concluding in one case that it was a dream (occurring in mental space) and in the other that it was “real” (occurring in physical space).
LaBerge and DeGracia have recently developed a formal approach to modeling the mental set of subjects during metachoric experiences such as OBEs and lucid dreams (22, 23). Any such mental set incorporates at least three components operating at distinct psychological levels: (a) a “reference-to-state,” which is the metacognitive recognition that the current state of consciousness is different than the usual waking state, (b) a “semantic framework,” which is the belief system used to conceptualize the nature of the experience and (c) a “goal-options context” consisting of methods of entry into and actions within the experience. This model provides improved understanding of the similarities and differences between lucid dreams and OBEs.
During both OBEs and lucid dreams, the individuals involved recognize that their state of consciousness differs from the normal waking state. The usual claim is that the experience is not a dream. However, the apparent intention of this statement is to assert that the event was real, not that it occurred in normal waking consciousness. Thus, the “reference-to-state” aspect of the mental set is identical in lucid dreams and OBEs.
In addition, published methods of inducing OBEs and lucid dreams, part of the “goal-option” aspect of mental set, are remarkable similar (see 8, 41, and 42). OBE and astral projection enthusiasts readily agree that times of transition between sleep and waking are fruitful for producing these events. On the other hand, the second part of the “goal-option” thought processes, the actions chosen in the experience, is likely to be of a different nature in a lucid dream than in an OBE. Because lucid dreamers do not believe they are interacting with the physical world, they are less concerned with such matters as social rules and physical limitations and tend to act in accordance with the belief that the environment is a figment of their imagination. Those who believe they are in an OBE tend to focus on the apparent reality of their surroundings, showing concern for whether others perceive them, attempting to move “physical” objects with the “astral body,” and seeking ways to prove they were really out-of-body.
These differences in action (goal-options) illustrate the primary factor distinguishing OBEs from lucid dreams: the interpretation of the experience or semantic framework. The thought process of trained lucid dreamers such as those in Study 1 entering OBE-like states generally follows the pattern, “I am now entering REM sleep, and I will soon be in a lucid dream,” acknowledging that a transition is occurring from one state of consciousness to another and that the sensory experiences in the new state will occur entirely in mental space. Most people, however, are not trained lucid dreamers, and are neither knowledgeable about the nature of transitions between states of consciousness nor experienced in identifying the qualities distinguishing waking from dreaming. As mentioned above, the default belief everyone holds while dreaming is that the experience is occurring in the waking state. Without experience in lucid dreaming, which provides insight into the intense sensory realism possible in dreams, and into the difficulty of determining whether one is dreaming or awake, most people will normally assume that the events they are experiencing are “real,” that is, occurring in the physical world. In the case of OBEs, while those having the experience possess the unusual cognition that they are not in the normal state of consciousness, the default belief is still that the events are real. There is nothing unusual or pathological about the tendency of a typical individual to take an OBE at face value; this simply reflects the knowledge base and belief structure (e.g., semantic framework) of the individual undergoing the experience. The origin of the semantic framework is the previous education and experience of the individual.
Since most people who have OBEs are not trained observers, educational background is likely to play a role in lack of critical thinking about the experience. However, a decrease in the quality of cognition may also contribute to lapses in logic. The three components of mental set discussed above are all psychological variables: they operate within the cognitive processes of the individual. Consistent functioning of these psychological mechanisms, however, depends on another variable, intact cognitive ability. Normal dreams are often characterized by uneven cognitive activity, varying from a high degree of critical mindedness to unthinking acceptance of the outrageous and illogical. The maintenance of a consistent mental set during a metachoric experience requires a high level of cognitive function, regardless of whether the semantic framework utilized is literally true. Thus, OBEs and lucid dreams may additionally share a common feature of occurring during brain states that can support sustained coherent thought. When a nonlucid dreamer passes through a variety of inconsistent semantic frameworks (see examples in 43), the cause may be a condition of relatively brain activity incapable of supporting coherent cognition.
The consistency of thought in these states is not perfect, however. In both lucid dreams (44) and OBEs, people often display lapses in critical thinking. For example, upon returning to normal waking consciousness after an OBE, people often recognize that anomalies were present in the OBE environment that indicated it was not the physical world. D. Scott Rogo, who wrote about OBEs, provided personal examples of post hoc recognition of OBE anomalies (8) that convinced him that the OBEs occurred in a world that was only a replica of the real world. Blackmore (2) names 11 similarities between OBEs and lucid dreams, one of which is: “The simplifications, distortions, and additions found in the experienced world can be similar in both experiences,” (p. 374). Blackmore gives an example from Green (30), in which a man while “out of body” saw a chimney stack on his house where there was none in reality, and describes her own out-of-body perceptions of stylized, simplified imagery. LaBerge (16) discusses a number of lapses of rationality experienced by people having OBEs. For example, one “astral projector” said that after exploring his house, he decided to return to his bedroom, thinking “I’ll look at myself on the bed.” (p. 232) But when he looked, he saw his mother, who “had been passed over quite a long time.” Curiously, finding his dead mother in bed in place of his sleeping body did not lead him to the conclusion that he was dreaming; instead he took this to mean that his mother's spirit would always be with him whenever he was “projected.” This sort of defective cognition seems quite typical of OBEs.
Higher levels of cerebral activation may also contribute to the greater perceived “realness” of OBEs when compared to ordinary dreams. Blackmore (2) notes that the stylization and simplification anomalies characteristic of OBEs are consistent with the modifications of perception found in recreations from memory. If the experience is hallucinatory, that is, not driven by sensory input, then it must be constructed from memory. Memories of familiar scenes are more likely to be accurate than memories of places seen more rarely. In addition, increased brain activation resulting in enhanced cognitive function may increase perceptual vividness and more effective representation of remembered perceptions.
One more dimension that helps to categorize a metachoric experience is lucidity. Lucidity refers to accurate recognition of one's true state of consciousness, e.g. asleep versus awake. LaBerge et al (37) have demonstrated that the onset of lucidity during REMsleep dreaming requires a high degree of autonomic activity. Autonomic arousal is an indirect physiological marker for cerebral activation. The similarities between OBEs and lucid dreams suggest that a similar degree of cerebral activation is present in both types of experience. The semantic framework in OBEs, however, prevents the person having the experience from recognizing the perceived environment as a mental construction and the state as a dream. As discussed previously, OBEs usually contain incongruous elements that could act as cues to lucidity for the prepared mind. Changing one's semantic framework, however, is a difficult task, requiring conscious reflection on the context of an experience. The default is to accept the semantic framework with which one is most familiar, the waking state.
The ability to identify the seamless transition from the waking state to dreaming typical of OBEs such as those reported in Study 1 is possible only with prior knowledge of the potential both for directly entering REM sleep from waking and for being aware that one is dreaming. Without this knowledge, the assumption that the entire experience occurs in the physical world is wholly natural.
Knowledge about REM-sleep physiology contributes to understanding the phenomena that often precede OBEs and sleep paralysis. REM-sleep onset is characterized by the initiation of cortically-derived descending paralysis of the skeletal muscles (excepting the extraocular muscles and those involved in respiration), and attenuation of cortical processing of information from the peripheral sense organs (47), in the context of a highly activated cerebral cortex. The sensation of leaving the body is often preceded by feelings of heaviness or paralysis in the body or body distortions. These events may arise from a lack of synchrony in the onset of muscular paralysis and sensory attenuation. If paralysis sets in while the mind is still processing proprioceptive information, the sleeper may actually feel paralyzed or feel a sensation of melting or increased heaviness in the limbs. The origin of electrical or whole body vibration sensations remains a mystery, but the explanation is likely to be related to the interaction between the sensory systems and the development of muscle atonia during the transition to REM sleep.
Furthermore, the perception of the onset of paralysis followed by the termination of somatosensory input from the body may account for the convincing sensation of “leaving the body.” First, the body begins to feel heavy or immovable. Next, the “heavy” sensation vanishes as sensory input is attenuated. However, loss of somatosensory input does not lead to elimination of the perception of a body. The brain continues to model a body image. The only change the mind perceives is the sudden feeling of lightness, easily interpretable as buoyancy, leading to the astonishing experience of floating to the ceiling. This is an example of the anchoring phenomenon observed in physiological psychology, in which a perception appears greater or lesser depending on the previous sensation. An everyday waking example of this occurs when one lifts an empty milk carton with the expectation that it is full. The carton seems to propel itself upward with a mysterious force. The newly out-of-body consciousness is aware of having been lying in bed just a moment ago. It is easier to believe one has left the body behind, and is now in an ethereal discorporate form, than that the body itself, so immobile just a moment ago, has suddenly become weightless.
The perception of an “out-of-body” body is part of the same general process that creates a realistic world in dreams. Neuroscientists are discovering that the brain creates “maps” of perceptual experience arranged topographically on the cortex (18-21). Because of these maps, the brain does not need to create each experience de novo. Perceptual mapping provides a mechanism for the processes described by LaBerge as “schemas.” (41) Schemas are maps of reality created by past experience that allow minds to predict what behavior is appropriate to a certain situation. Schemas also determine the interpretation of ambiguous stimuli.
The perceptual maps activated along with the current mental schema fill in blanks left by ambiguity with features predicted by the schema. For example, amputees often feel pain and cramping that their brains attribute to the limb that is no longer present. The ambiguous stimulus is neuronal activity somewhere along the pathway of sensory input from the missing limb to the cerebral cortex. The sudden loss of a limb does not cause loss of the limb's representation in the brain's map of the body. Therefore the brain's best interpretation of the neuronal information is that it is coming from that limb. In dreams, all of the sensory input from the body has been lost. Brain activity persists and activates the normal perceptual maps that create the experience of a body. In fully realistic dream bodies, dreamers freely travel about in fully realistic dream worlds. Thus, one could reasonably say, using the definition of OBEs provided at the beginning of this paper, that all dreams are OBEs. Indeed, this was exactly the position taken by Muldoon in his writings on astral projection, although he believed that all dreamers were in astral bodies traveling on the astral plane (4).
Some people, however, report not being aware of having a body in dreams, and in Alvarado's (48) survey of OBEs, only 23% of people who had OBEs reported an “out-of-body” body similar to the physical one. Interestingly, this observation supports the applicability of another finding regarding the mapping of experience in the brain. The representation of “allocentric space” (defined as the external environment in which the observed is embedded) appears to involve different cerebral networks than the representation of “egocentric space” (the localization of the site of conscious experience) (49). Independent activation of these representations could lead to experiences such as perceiving an environment but not a body image, or perceiving one's locus of awareness as being separate from the body.
This analysis has focused on OBEs that occur in the REM sleep state. However, evidence suggests (1, 31) that OBEs can occur in states other than REM, albeit more rarely. OBEs have been associated with trance and meditative states, drug-induced states, sensory deprivation, hypnopompic and hypnagogic states, high stress conditions (e.g. near-death-like phenomena associated with cardiac arrest), and fainting (10). As discussed earlier, any state that combines a high level of cortical activation with diminished awareness of the body may be conducive to out-of-body experiences. REM sleep may not be necessary in light of Irwin's (45) proposal that a high capacity for absorption may allow a person to focus so much attention on a mental that too little attentional capacity is left over to consciously perceive sensory input from the body. High states of arousal may further decrease the capacity to process both the mental image and the body, thus the more interesting or potentially threatening experience would prevail in consciousness—in this case, the feeling of being out of body (46).
To further blur the boundaries between dreaming and waking experience, consider the idea proposed by LaBerge (41) and Llinas (21) that all perceptual experience is constructed by the brain. At some threshold of cerebral activity, the topographical cortical “maps” become active resulting in conscious experience of an external world, a body image, and a self. In the waking state, the brain attends to information from the sensory organs reporting on conditions in the physical world, and uses that information to modify the “reality” it constructs. The only difference between the world constructed in the waking state from that constructed in dreams is the degree to which sensory input constrains what is perceived. Because our brains cannot directly perceive reality but rather create the worlds we live in using data from our sense organs which is heavily modified by central processes, the term “metachoric” may apply to all of experience. If dreaming and waking are not totally different states of consciousness as most have assumed over the ages, then an extraordinary shift in our perspective on illusion and reality is in order. Being awake can no longer refer to being aware of “the real world,” and “ asleep” can no longer be synonymous with “unconscious.” As LaBerge wrote a decade ago (50):
“As long as we continue to consider wakefulness and sleep as a simple dichotomy, we will lie in a Procrustean bed that is bound at times to be most uncomfortable. There must be degrees of being awake just as there are degrees of being asleep (i.e. the conventional sleep stages). Before finding our way out of this muddle, we will probably need to characterize a wider variety of states of consciousness than those few currently distinguished (e.g. 'dreaming,' 'sleeping,' 'waking,' and so on).” (p. 124)
The results from the present study lead to some testable predictions. People who experience rapid transitions from waking into REM sleep, such as narcoleptics, should report more OBE-like phenomena than the general population. The frequency with which people experience WILDs should strongly correlate to OBE frequency. OBEs are likely to arise whenever decreased somatosensory input occurs in the context of persistent high levels of cognitive function. It may be possible to create such conditions using pharmacological agents such as dissociative anesthetics that block sensory input while increasing cortical activity.
In conclusion, the data and analysis presented here argue that out-of-body experiences are mental events that arise out of the same physiological conditions as wakeinitiated lucid dreams. Both involve transitions waking to dreaming, and are accompanied by similar phenomenology such as vibrations, unusual auditory hallucinations, sleep paralysis, and a sensation of floating out of body. Using the proposed model for understanding metachoric experiences reveals that the difference between OBEs and lucid dreams lies solely in the semantic frameworks used. In the end, we suggest that in approaching the study of consciousness, the most fruitful approach may require us to abandon arbitrary distinctions between states and to recognize that all conscious experience derives from the activity of the brain. The primary function of the forebrain is the creation of complex models of reality that allow us to accurately predict the outcome of our interactions with the physical world. This function does not cease with the onset of sleep and is not dependent on external input to the sense organs.
In a final note, we would like to address the concerns of those for whom OBEs have provided revelation of existence beyond the limits of the physical body. Declaring OBEs dreams does not diminish their reality if, by the same argument, we declare that waking reality is a dream as well! The worlds we create in dreams and OBEs are as real as this one, and, further, they are unfettered by the constraints of the physical universe. In dreams, we have the potential to explore the true powers of the mind without the limitations imposed in the “real world” by the need to survive in a hostile environment. How much more exhilarating it must be to be “out-of-body” in a world where the only limit is the imagination, than to be loose in the physical world in a powerless body of ether! Freed of the constraints imposed by the physical, expanded by the knowledge that we can transcend all previously known limitations, who knows what we could be, or become?
Acknowledgements
We thank the Fetzer Institute, the Institute of Noetic Sciences, and Kenny Felder for financial support, and Mushkil Gusha for the usual help.
References
1. Blackmore S. Beyond the body London: Granada; 1983.
2. Blackmore S. A theory of lucid dreams and OBEs. In: Gackenbach J, LaBerge S, eds. Conscious Mind, Sleeping Brain. New York: Plenum; 1988:373-387.
3. Leadbeater CW. The Astral Plane.(12 th reprint, 1984). Madras: Vasanta Press; 1895.
4. Muldoon S, Carrington H. The Projection of the Astral Body New York: Samuel Weiser; 1974.
5. DeGracia DJ. Les paradigmes de la conscience dans le sommeil. Rêver. 1997; 1(3):26-35. Online: http://wwwusers.imaginet.fr /~ghibelli/dondega.html.
6. Alvarado CS. Recent OBE detection studies: A review. Theta. 1982;10:35-37.
7. Monroe R. Journeys out of the Body. Garden City, NY: Doubleday, 1971.
8. Rogo DS. Leaving The Body. New York: Prentice Hall, 1986.
9. Green C & McCreery C. Apparitions. London: Hamish Hamilton, 1975.
10. Alvarado CS. Out-of-Body Experiences. In Cardea E., Lynn SJ, & Krippner S. (eds.) Varieties of Anomalous Experience. Washington, DC: American Psychological Association.
11. Black D. Ekstasy: Out of the Body Experiences. New York: Bobbs-Merrill, 1975.
12. Palmer J. The out-of-the body experience: A psychological theory. Parapsychology Review, 1978;9(5):19-22.
13. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Association, 1994.
14. Gabbard GO, Twemlow SW. With the eyes of the mind New York: Praeger; 1984.
15. LaBerge S. Lucid dreaming as a learnable skill: A case study. Perceptual and Motor Skills. 1980;51:1039-1042.
16. LaBerge S. Lucid dreaming Los Angeles: J.P. Tarcher; 1985.
17. LaBerge S, Levitan L, Brylowski A, Dement W. “Out-of-body” experiences occurring during REM sleep. Sleep Research. 1988;17:115.
18. Cline HT. Topographic maps: Developing roles of synaptic plasticity. Current Biology 1998;8:R836- R839.
19. Kaas JH. Topographic maps are fundamental to sensory processing. Brain Research Bulletin. 1997;44:107-112.
20. O'Keefe J. A computational theory of the hippocampal cognitive map. Progress in Brain Research.. 1990;83:301-312.
21. Llinas R., & Pare D. Of dreaming and wakefulness. Neuroscience. 1991;44:521-535.
22. DeGracia DJ & LaBerge S. In the theater of dreams: global workspace theory, dreaming, and consciousness. Consciousness and Cognition. In submission.
23. LaBerge S & DeGracia DJ. Varieties of lucid dreaming experience. In Kunzendorf RG and Wallace B (eds), Individual Differences in Conscious Experience. Philadelphia, John Benjamins Publishing Company. In Press 1/99.
24. Irwin HJ. Out-of-the-body experiences and dream lucidity. In: Gackenbach J, LaBerge S, eds. Conscious Mind, Sleeping Brain. New York: Plenum; 1988:353-371.
25. Salley RD. REM sleep phenomena during out-of-body experiences. Journal of the American Society for Psychical Research. 1982;76:157-165.
26. Hishikawa Y, Shimizu T. Physiology of REM sleep, cataplexy, and sleep paralysis. Advances in Neurology. 1995;67:245-271.
27. Everett HC. Sleep paralysis in medical students. Journal of Nervous and Mental Disease. 1963;136:283-287.
28. Mahowals MW & Schenck CH. Dissociated states of wakefulness and sleep. Neurology. 1992;42:suppl 6:44-52.
29. Blackmore S. A postal survey of OBEs and other experiences. Journal of the Society for Psychical Research. 1984;52:227-244.
30. Green CE. Out-of-the-body experiences London: Hamish Hamilton; 1968.
31. Poynton JC. Results of an out-of-the-body survey. In: Poynton JC, ed. Parapsychology in South Africa. Johannesburg: South African Society for Psychical Research; 1975.
32. Is ESP Perceiving or Remembering? Parapsychology Review. 1979;10(4):23-27.
33. Schneck JM. Sleep paralysis and spontaneous hypnotic paralysis. Perceptual and Motor Skills. 1970;31(1):16.
34. Spector M, Bourke DL. Anesthesia, sleep paralysis, and physostigmine. Anesthesiology. 1977;46:296-297.
35. Glicksohn J. The structure of subjective experience: Interdependencies along the sleepwakefulness continuum. Journal of Mental Imagery. 1989;13(2):99-106.
36. LaBerge S, Nagel L, Dement WC, Zarcone V. Lucid dreaming verified by volitional communication during REM sleep. Perceptual and Motor Skills. 1981;52:727-732.
37. LaBerge S, Levitan L, Dement WC. Lucid dreaming: Physiological correlates of consciousness during REM sleep. Special Issue: Cognition and dream research. Journal of Mind & Behavior. 1986;7(2-3):251-258.
38. Rechtschaffen A & Kales A (Ed). A manual of standardized terminology, techniques and scoring system for sleep stages of human subjects. Los Angeles: Brain Information Service/Brain Research Institute, UCLA, 1968.
39. Olson M. The incidence of out-of-body experiences in hospitalized patients. Journal of Near- Death Studies. 1988;6(3):169-174.
40. Crookall R. Case-book of astral projection. Seraucus, NJ: University Books, 1972.
41. LaBerge S. & Rheingold H. Exploring the world of lucid dreaming. New York: Ballantine Books, 1990.
42. Ophiel. The art and practice of astral projection. York Beach, Maine: Samuel Wiser, Inc., 1982.
43. Hobson JA. The dreaming brain. New York: Basic Books, 1988.
44. Levitan L. A fool’s guide to lucid dreaming. Nightlight 1994;6:1-5. Online: http://www.lucidity.com/NL62.FoolsGuide.html.
45. Irwin HJ. Some psychological dimensions of the out-of-body experience. Parapsychology Review. 1981;12:1-6.
46. Eysenck MW. Attention and arousal Berlin: Springer-Verlag; 1982.
47. Velasco F, Velasco M, Cepeda C, & Munoz H. Wakefulness-sleep modulation of cortical and subcortical somatic evoked potentials in man. Electroencephalography and Clinical Neurophysiology 1980;48:64-72.
48. Alvarado CS. ESP during spontaneous out-of-body experiences: A research and methodological note. Journal of the Society for Psychical Research. 1986;53(804):393-397
49. Maguire EA. Hippocampal involvement in human topographical memory: evidence from functional imaging. Philosophical Transactions of the Royal Society of London - Series B: Biological Sciences. 1997; 352(1360):1475-80.
50. LaBerge, S. Lucid dreaming: Psychophysiological studies of consciousness during REM sleep. In Bootzen, R.R., Kihlstrom, J.F. & Schacter, D.L., (Eds.) Sleep and Cognition. Washington, D.C.: American Psychological Association, 1990 (pp. 109-126).